

HRT and Menopause
Legacy of the Women's Health Initiative

*Note: Linked here is an excellent article that is more comprehensive and analytical than what I plan to write in this post. I am setting out only to summarize and make more digestible an important topic that is under appreciated by both the public and many medical professionals.
Since 2002, the percentage of U.S. women taking hormone replacement therapy (HRT) for menopause has fallen by roughly 50%. This dramatic decline was largely due to reports that emerged from the Women’s Health Initiative (WHI) suggesting the use of HRT increased the risk of breast cancer. This post will provide a summary of the history of HRT as well as the claims, flaws, and legacy of the WHI.
The average age of onset of menopause is 51 years. When a woman’s ovaries are depleted, they shut down, leading to a rapid decline of estrogen. While some fortunate women may experience few if any symptoms, many suffer from hot flashes, night sweats, palpitations, depression, joint pain, cognitive decline, and many more symptoms. Around the middle of the 20th century, researchers developed the ability to extract estrogen from the urine of pregnant mares (horses). Thus Premarin (PREgnant MARes’ urINe), the first estrogen tablets, came into existence.
It was later found that postmenopausal women taking estrogen had a significant increase in the risk of uterine cancer. In hindsight this was entirely predictable, for some context here is a brief and simplified version of why this risk of cancer makes sense:
During a woman’s reproductive years, estrogen stimulates the endometrium of the uterus to proliferate, creating the substrate for implantation of a fertilized egg. After ovulation, progesterone becomes the dominant hormone that maintains and fine tunes the uterine tissue to enable pregnancy. In the absence of a fertilized egg, the lining of the uterus is shed, and the cycle begins anew. See below a useful schematic of the menstrual cycle.

When postmenopausal women were given estrogen alone, that led to proliferation of the endometrium, and without the natural counterbalance of progesterone and menses, a higher risk of cancer. When progestin (synthetic progesterone) was added to HRT the increased risk of uterine cancer was negated. Around 16 million women in the United States were taking HRT in 2002.
Everything changed when the Women’s Health Initiative halted their trial on the use of HRT in postmenopausal women due to an increased risk of breast cancer. The study was meant to establish whether the use of HRT improved cardiovascular health. The primary outcome was coronary heart disease (CHD) and it had a primary adverse event of invasive breast cancer. The study was halted after a mean follow-up of 5.2 years.
They reported an estimated hazard ratio of 1.26, suggesting that women given HRT (estrogen plus progestin) had a 26% increase in risk of developing breast cancer. Importantly, the increase in risk was not statistically significant when the study was stopped. If we zoom in on this finding, we can see that in the women randomized to HRT in this trial, 166 out of 8,506 developed invasive breast cancer. In the placebo group, 124 out of 8,102 developed invasive breast cancer. In other words, just under 2% of women receiving HRT and just over 1.5% of women receiving placebo. The increase in absolute risk of invasive breast cancer was 0.42%. Put simply, they had a non-statistically significant finding that for every 238 women given HRT, one would develop invasive breast cancer that otherwise wouldn’t have.
That is a much less alarming result than those that were plastered on newspapers across the country. The next thing to consider is the characteristics of the study population. The average age of the women in the trial was 63. Yes, over a decade past the average age of onset of menopause. 70% of the women were either overweight or obese, 50% were either former or current smokers, and over a third had hypertension. Additionally, the study explicitly discouraged enrollment of women with moderate to severe postmenopausal symptoms.
The reason the study population had these characteristics is because the purpose of the study was to determine whether or not HRT is protective in heart disease, not its effect on women that have recently entered menopause. An older, largely overweight/obese population with high rates of smoking and hypertension is ideal for analyzing cardiovascular risk. Additionally, if many of the women had symptoms of menopause, the ones randomized to placebo would be more likely to drop out due to those symptoms, so while the selection made sense in the context of the study, it’s generalizability to all women is weak.
The extrapolation of this study and its ostensible findings to all postmenopausal women has been one of the more tragic results of poorly interpreted data. The meme that “Estrogen causes breast cancer” is widespread, the data behind it is anemic. In fact, the estrogen-only arm of the WHI, consisting of women with prior hysterectomies, found no increased risk of breast cancer.
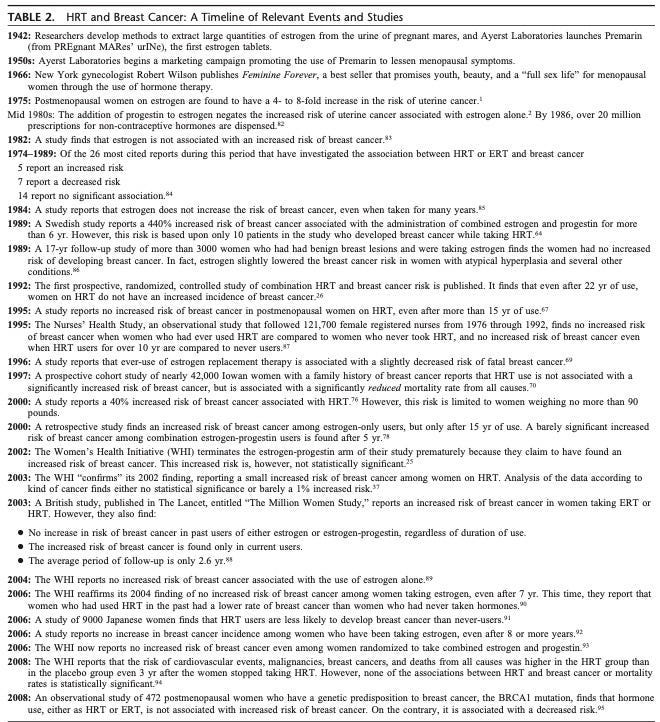
HRT and Breast Cancer: The table below is from the paper I linked to at the top, “Hormone Replacement Therapy: Real Concerns and False Alarms” authored by Avrum Bluming, M.D., and Carol Tavris, Ph.D. I highly recommend reading the paper, as well as the book they wrote together on this very topic, “Estrogen Matters”.
HRT in Breast Cancer Survivors:
From 1980 to 2008, twenty studies were published on the use of HRT in women with a history of breast cancer. Only one found an increase in risk of breast cancer with use of HRT, and this was only true with concurrent use of tamoxifen. Previous breast cancer is commonly cited as a contraindication to HRT, which is unwarranted.
Aside from breast cancer, the 2002 WHI report claimed HRT led to an increased risk of cardiovascular disease and a decreased risk of fractures. We will briefly address these two topics.
Cardiovascular Health:
Women are more likely to die of heart disease than breast cancer in every decade of their life. Often things like heart attacks are thought of as classically afflicting men, and women are more likely to be concerned with developing breast cancer. There is robust literature suggesting estrogen has a protective effect against cardiovascular disease. So how could the WHI find an increase of CHD in those given HRT?
This brings us back to the population that was studied. HRT is protective when given early, in women entering menopause up to around 6 years after menopause. The protective effect weakens with increasing time between menopause and initiation of HRT, after 10 years this can turn into an increase in risk, at least for the first year on HRT. It is thought that while estrogen may delay to development of atherosclerotic plaques, reintroduction of estrogen in the context of established disease can temporarily increase the likelihood of rupture of said plaques. Remember the average woman in the WHI study was over a decade post menopause and at high risk of cardiovascular disease (overweight/obese, smoking status, hypertension rates). Once again, generalizability to all women is not reasonable.
Bones:
There is no argument about the beneficial effect of estrogen on bone health. Fractures, especially of the hip, represent a significant concern to the health of women as they age. The WHI itself reported a 33% decrease in hip fractures among women randomized to HRT. This protective effect is most significant in women at high risk of osteoporosis.
Summary:
The use of HRT, just like any other medical intervention, must be based on individualized cost-benefit analysis. Poor interpretation of trial data has led to a halving of the rate of HRT use in women. Menopausal symptoms can be debilitating and may persist for many years. HRT represents a valuable therapeutic tool, best realized when started early. The WHI rushed into publication based on a non-statistically significant finding in a population that bears no resemblance to the average woman entering menopause in her early fifties. The original claims about an increased risk of breast cancer and heart disease have been unable to stand the test of time. HRT has been shown to not only prevent the needless suffering of women but also has the potential to extend lifespan.