
Gender Trends

I’ve been meaning to revisit the topic of Gender Therapy, and a recent study published by the American Academy of Pediatrics (AAP) offers a useful entry into this space. Jack Turban, MD, MHS was the lead author of the study, entitled “Sex Assigned at Birth Ratio Among Transgender and Gender Diverse Adolescents in the United States”.
This study is an example of what happens when advocacy preempts scientific rigor. The reasoning behind the study went something like this: Gender clinics have reported increasing rates of persons presenting with gender dysphoria, and this increase has been noted to be disproportionately seen in females relative to males. Many observers of this trend have suggested this might be best explained by a social phenomenon referred to as “social contagion”. This phenomenon has been used in some US states as justification for limiting “Gender-Affirming” medical care. The authors sought to examine national CDC data to analyze this supposed trend. I believe their intentions were good, if not their study.
They used CDC survey data from two years, 2017 and 2019, and compared the ratio of males to females that reported being transgender. Even if the data set they used was robust, two data points with only 2 years between them is clearly not going to give us much confidence in anything. The data set was also quite poor. This was essentially a study of the state of Maryland, as has been pointed out by a group of researchers in the field. Here is the critique of their analysis, if you open the original study it is included in the comments section at length, just scroll to the bottom.
Note: AMAB=Assigned Male at Birth, AFAB=Assigned Female at Birth
This study was exceptionally poor; it’s unclear why the AAP saw fit to publish it. To understand the debate behind a study like this we have to talk about Lisa Littman, MD, MPH. A fun fact I recently learned is that she completed her MPH and Residency in Preventative Medicine at Mount Sinai. Anyways, she published a study in 2018 that sparked a fire. The original study was called “Rapid-onset gender dysphoria in adolescents and young adults: A study of parental reports”.
She had observed many individual parents reporting that their adolescent children were suddenly experiencing gender dysphoria with no prior history, often occurring in multiple adolescents within friend groups. If you read my first post on this topic, you have seen that historically, individuals with gender dysphoria have presented as young children, well before puberty. So she conducted a survey, and coined the term “rapid-onset gender dysphoria” (ROGD). I encourage you to read the original study linked above. It is quite long, roughly pages 5-30 detail the procedure, measures, and results. The introduction, background, discussion and conclusion are worth reading if you don’t have time for the M&M.
The backlash that Dr. Littman faced was swift and furious. I previously said “original study” because after the post-publication backlash, the journal (PLoS-One) re-published the paper with an altered title, abstract, introduction, discussion, and conclusion sections. The “corrected” title is “Parent reports of adolescents and young adults perceived to show signs of a rapid onset of gender dysphoria”. Here is the correction statement and updated study link. It amazes me that this study was so heavily edited. It’s one thing if you make an author change some kind of egregious mistake, but this looks to me like a scientific journal’s genuflection to activists.
Brown University, where Dr. Littman was at the time, removed its press release about the paper and publicly apologized. PLoS One’s editor in chief apologized as well, and as noted the journal issued a correction. Activists found out that Dr. Littman worked as a part-time consultant at the Rhode Island Department of Health, and under sufficient pressure the DOH severed ties. As I write in 2022 this kind of institutional cowardice is an old and familiar story. Dr. Littman observed reports of atypical, clustered presentations of gender dysphoria. She researched this phenomenon and published her findings and hypotheses. That was seen as beyond the pale.
Her hypotheses regarding the factors contributing to the possible social contagion effect roughly came down to this:
The belief that non-specific symptoms should be perceived as gender dysphoria and that their presence is proof of being transgender
The belief that the only path to happiness is transition
The belief that anyone who disagrees with the self-assessment of being transgender or opposes the plan for transition is transphobic, abusive, and should be cut off
Note: I have used Abigail Shrier’s “Irreversible Damage” as a reference for some details of Dr. Littman’s experience. This book is indispensable for anyone wishing to understand the critique of where the US is heading on this topic.
What can we say about the presence or absence of trends in persons presenting with gender dysphoria?
A 2015 paper analyzed trends from two clinics. One in Toronto, another in Amsterdam.
Toronto: From 1999-2005, 36 males and 17 females were referred for gender dysphoria. The Sex Ratio was 2.22:1 (M:F). From 2006-2013, 73 males and 129 females were referred for gender dysphoria. The Sex Ratio was 1:1.76 (M:F). This clinic saw an increase in overall referrals as well as an inversion of the ratio of males to females during this time.
Amsterdam: From 1989-2005, 109 males and 77 females were referred. Sex Ratio was 1.41:1 (M:F). From 2006-2013, 86 males and 148 females were referred. Sex Ratio was 1:1.72 (M:F). This clinic saw an increase in overall referrals as well as an inversion of the ratio of males to females during this time.
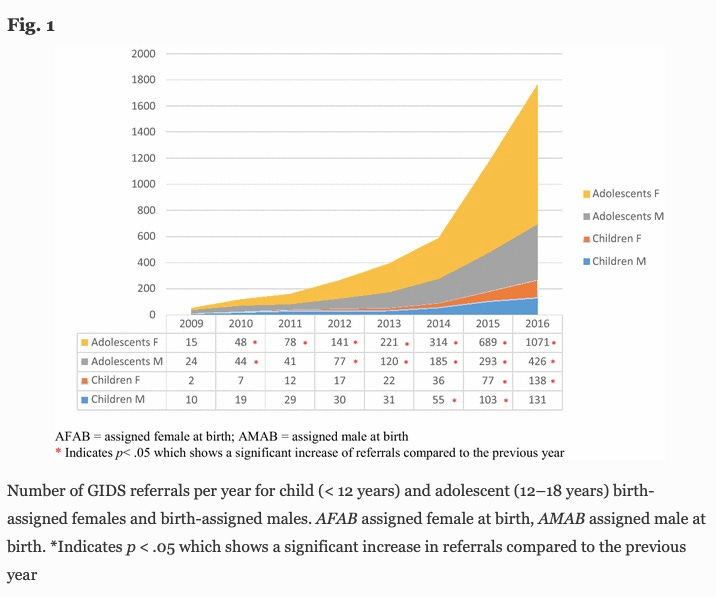
A 2018 paper looked at the national Gender Identity Development Service (GIDS) in the UK, the largest child and adolescent specialist gender service in the world. GIDS is part of the Tavistock clinic in London.
From 2009-2016, referrals were tracked by age and sex. Children were considered <12 years old, adolescents were considered 12-18 years old.
Male children increased from 10 in 2009 to 131 in 2016.
Female children increased from 2 in 2009 to 138 in 2016.
Male adolescents increased from 24 in 2009 to 426 in 2016.
Female adolescents increased from 15 in 2009 to 1,071 in 2016.
Here we see a dramatic increase in referrals across the board with adolescent females disproportionately represented. Here is the graphic:
A recent report in 2019 from the UK has shown referrals began leveling off around 2018-2019.
The American Association of Plastic Surgeons don’t provide data on patient age in their annual reports, but we can observe trends in gender confirmation surgeries.
From 2016-2017, Male-to-Female surgeries increased from 1,759 to 2,483 (41% increase). Female-to-Male surgeries increased from 1,497 to 5,821 (289% increase).
From 2019-2020, Male-to-Female surgeries increased from 5,616 to 6,368 (13% increase). Female-to-Male surgeries increased from 8,986 to 9,985 (11% increase).
Note: The surgery data gives no data on patient age, and I do not mean to imply that these surgeries are happening in minors, I don’t know what the demographics are and may dedicate some future post to the surgical side of this topic, which is clearly fraught when minors are involved. It is also worth pointing out that a single individual can have multiple surgeries when transitioning. I will say this alone for now: In 2019 the US sex-reassignment surgery market size was valued at $267 million. I expect that number to double in the next decade. Here is a list of the most prominent players in this market.

Moving Forward: We have seen a bad study, a researcher unfairly maligned, and some suggestive trends. I will turn back to the Tavistock clinic in the UK. Just over a week ago the NHS announced the impending closure of the GIDS Tavistock clinic after more than 30 years of existence. Here is an excellent piece by Lisa Selin Davis in Common Sense. I highly recommend reading it, as I don’t intend to regurgitate the information. I will share some of the main points.
This represents another trend that is bizarrely underreported in the United States. European countries that previously administered “gender-affirming care” have dramatically revised their policy.
Sweden: Sweden’s National Board of Health and Welfare released new guidelines for treating young people with gender dysphoria earlier this year. The new guidelines state that the risks of these “gender-affirming” medical interventions “currently outweigh the possible benefits, and that the treatments should be offered only in exceptional cases.”
Finland: Finland’s Council for Choices in Health Care (COHERE) came to a similar conclusion a year earlier, noting: “The first-line intervention for gender variance during childhood and adolescent years is psychosocial support and, as necessary, gender-explorative therapy and treatment for comorbid psychiatric disorders.” And: “In light of available evidence, gender reassignment of minors is an experimental practice.” Gender reassignment medical interventions “must be done with a great deal of caution, and no irreversible treatment should be initiated.”
UK: The interim report of the Cass Review, largely attributed to leading the NHS to close the Tavistock Clinic, had this to say, “Much of the existing literature about natural history and treatment outcomes for gender dysphoria in childhood is based on a case-mix of predominantly birth-registered males presenting in early childhood. There is much less data on the more recent case-mix of predominantly birth-registered females presenting in early teens, particularly in relation to treatment and outcomes.”
Final Thoughts: I worry that in the United States our culture war has and will continue to make appropriate decisions regarding gender therapy difficult. Nothing is more important than protecting the health of children. Where are the medical institutions standing up and addressing the lack of data behind these therapies? I understand some people believe that calling attention to the problems in this space will make it harder for transgender persons to access care. I don’t think they appreciate that we don’t know whether this “care” is helping or hurting them.